
Help us improve our information
We need your help to improve our information to better support people with Crohn’s and Colitis. Fill in our short survey to let us know what we're doing well and how we can better meet your needs.
Diarrhoea is a common symptom of Crohn’s and Colitis. You may continue to have diarrhoea even when your Crohn's or Colitis is under control.
This information is for anyone with Crohn’s or Colitis (including Microscopic Colitis) who has diarrhoea. It may also be useful for those involved in their care. This information covers:

We need your help to improve our information to better support people with Crohn’s and Colitis. Fill in our short survey to let us know what we're doing well and how we can better meet your needs.
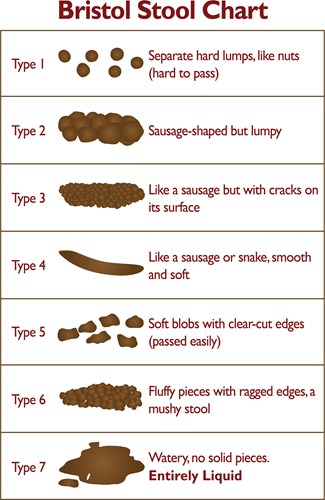
The Bristol Stool (Poo) Chart can be used to assess your poo. The 7-point scale helps describe the shape and texture of your poo. If your poo looks like types 1 or 2, it could mean that you have constipation. Experts generally consider types 3 and 4 to be healthy poos. Type 5 is considered healthy going towards diarrhoea. And types 6 or 7 suggest that you have diarrhoea.
Diarrhoea is when you have a loose or liquid poo three or more times a day, or more often than is usual for you.
Diarrhoea is one of the main symptoms of Crohn’s Disease, Ulcerative Colitis and Microscopic Colitis. About 8 in every 10 people with the conditions have diarrhoea at some point.
In people with Crohn’s or Colitis diarrhoea can be mixed with mucus, pus and blood. You may feel that you need to rush to the toilet. This is known as urgency. Or you may experience bowel incontinence.
Find out more about Bowel incontinence and urgency.
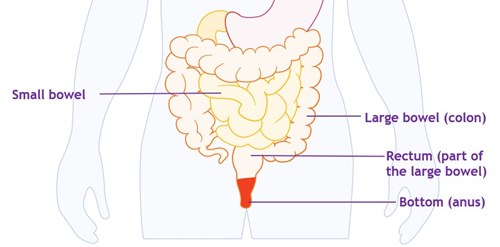
The small bowel absorbs the useful nutrients from what you have eaten. Then the liquid and non-digestible parts of food move into your colon. Usually, the colon absorbs most of the water, and the leftover waste forms a solid poo. This collects in the last part of the colon and the rectum before passing out of the body when you have a poo.
During a flare-up the cells that line the bowel become inflamed. This means that the bowel cannot absorb all the nutrients and water. This can cause watery poo, the need to poo more often and to get to the toilet quickly.
So, your diarrhoea might be due to a flare-up of your condition. But there are other factors that may be causing it or making it worse. These include:
5-ASAs (aminosalicylates) such as mesalazine can cause diarrhoea. Some immunosuppressants, including infliximab, mercaptopurine, and methotrexate, can also cause diarrhoea. It can be hard to tell if it is your condition or your treatment causing diarrhoea. Speak to your IBD team if you’re not sure what may be causing your symptoms.
Diarrhoea might also be a side effect of some medicines that you may be taking for other conditions. For example, acid-lowering treatments, such as omeprazole and lansoprazole, and antibiotics can cause diarrhoea. You can check the information leaflet that comes with your medicine to see if diarrhoea is a side effect.
In this surgery the colon is removed and the end of the small bowel (terminal ileum) is attached to the rectum. Because you no longer have a colon to absorb water, your poo may be quite watery. You may have to go to the toilet many times during the day and night.
Our information Surgery for Crohn’s Disease and Surgery for Ulcerative Colitis have more details about types of surgery for Crohn’s and Colitis.
Bile acids help you to digest fats. The liver makes bile acids when you eat and releases them into the small bowel. Most of the bile acids are re-absorbed in the last part of the small bowel, and returned to the liver. But, if part of your small bowel is inflamed or has been removed the bile acids are not re-absorbed. So, much higher levels of bile acids pass into the colon. This irritates the lining of the colon, which draws water into the colon causing diarrhoea.
If bile acid malabsorption is severe, you may not be able to digest fats from your food. So, the fats pass into your colon, causing your poo to become fatty. This is sometimes called steatorrhea. Fatty poo is greasy and runny and often smelly. It may float, so can be difficult to flush away.
If you have anaemia you may have iron supplements. Iron supplements usually cause constipation. But they can cause diarrhoea in some people.
People sometimes mistake IBS for Inflammatory Bowel Disease (IBD), but it is a different condition. Like Crohn's and Colitis, IBS can cause tummy pain, bloating, and loose or watery poo. But IBS does not cause inflammation of the bowel or bleeding. Some people with Crohn’s or Colitis develop IBS-like symptoms even when their Crohn's or Colitis is inactive.
Some people find that what they eat has little effect on their symptoms. Others find that certain foods trigger symptoms, and cutting down those foods helps. You could use a food diary or app to find out if any foods seem to affect your symptoms. It’s a good idea to discuss possible triggers with your IBD team or dietitian before making any big changes to your diet.
Changes in symptoms after eating certain foods does not always mean that your condition is flaring up. Food can sometimes trigger symptoms in people without Crohn’s or Colitis.
It is important not to cut foods out of your diet without talking to your dietitian or IBD team. It could mean you miss nutrients that your body needs.
See our Food information for more on diet.
Diarrhoea can be a sign of a tummy infection, such as gastroenteritis or Clostridium difficile.
Small-intestinal bacterial overgrowth (SIBO) is a condition where there are more bacteria in the small bowel than usual. These extra bacteria can cause symptoms such as diarrhoea, weight loss and malnutrition. This overgrowth occurs when food moves through the gut more slowly than usual. SIBO is often associated with Crohn’s and Colitis.
Mental health problems, like stress, can have a negative effect on gut symptoms.
Treatment for diarrhoea will depend on the cause. Often, the first step in managing diarrhoea is to get your Crohn’s or Colitis as well controlled as possible. Reducing the inflammation in your bowel should help to improve gut symptoms.
Medicines to control diarrhoea are often called anti-diarrhoeal medicines. There are different types of anti-diarrhoeal medicines. Which one you try will depend on a number of things, including the cause of your diarrhoea.
Antimotility medicines are a common type of anti-diarrhoeal medicine. Your doctor or IBD team may suggest these if you keep getting diarrhoea.
Antimotility medicines slow down you’re the movement of food through your gut. This means that food takes longer to pass through your gut. This allows more water to be absorbed from your bowel into your body. So, your poo becomes firmer, and you need to poo less often.
Loperamide is a commonly used antimotility medicine.
Always check with your IBD team before taking an antimotility medicine.
Bulk-forming laxatives are often used to treat constipation. But your doctor may also recommend them for diarrhoea. These include ispaghula and sterculia, which come as granules that you mix with water. They absorb water in the bowel, which makes your poo bulkier. This helps your bowels to keep moving and working normally.
Check with your pharmacist or IBD team before taking a bulk forming laxative. Do not take bulk-forming laxatives if you have a narrowing of the bowel, called a stricture.
Some drug manufacturers advise against using antimotility medicines or laxatives in people with acute or severe Crohn’s or Colitis. Your doctor or nurse may have prescribed these for you. If so, they will have considered the advantages and disadvantages of you taking them. Speak to your IBD team if you have any concerns about taking them.
These medicines relax the muscles in your gut. This eases painful cramps or spasms. They include:
Antispasmodic medicines can be useful in people with IBS-like symptoms.
Bile acid binders can be used for diarrhoea caused by bile acid malabsorption. They bind to bile acids in the small bowel. This stops the bile acids reaching the large bowel and causing diarrhoea. The main bile acid binders include colestyramine and colestipol. These come in powder or granule form and can be mixed with water, juice or soft food. A tablet form called colesevelam is also available.
Side effects include bloating and discomfort in the tummy, feeling sick and constipation. They can affect the absorption of other medicines that you might be taking. So, it is important to check with your IBD team or pharmacist how to manage taking them alongside each other.
Some people find that what they eat or drink has no effect on their diarrhoea. Others find that changing what they eat and drink helps. You could use a food diary or app to find out if any foods seem to affect your symptoms.
Foods or drinks that might make diarrhoea worse in people with or without Crohn’s or Colitis include:
Gluten is a protein that’s found in wheat, barley, rye and oats, or foods that contain them. If your diarrhoea is worse after eating foods containing gluten you may be sensitive to gluten. About 1 in 4 people with Crohn’s or Colitis say they are sensitive to gluten and avoid it in their diet. This might improve symptoms for some people, but there is not enough evidence to recommend it for everyone with Crohn’s or Colitis.
Sometimes, gluten sensitivity is a sign of coeliac disease. You can ask your GP for a blood test to check for this. Note that you should include gluten in your diet when you have the blood test. This is because avoiding it could lead to an incorrect result. More information about coeliac disease is available at www.coeliac.org.uk.
Current guidelines say that unless you have a narrowing (stricture) in your gut, you do not need to limit your fibre intake when your condition is under control.
But for some people high-fibre foods can make diarrhoea worse. And during flare-ups, it might help to reduce the amount of fibre you eat. Eat fibre that is easy to digest, like well-cooked, peeled vegetables, bananas, melons, or fruit juice.
Fibre is an important part of the diet, as it helps the bowel to function normally. So talk to your IBD team or dietitian before making changes to the fibre in your diet. You can try adding fibre back into your diet once your flare-up has settled.
Lactose is a sugar found in dairy products like milk, cream and cheese. An enzyme called lactase in the lining of your small bowel usually breaks it down so your body can absorb it.
If lactose is not broken down, your body cannot absorb it. This is called lactose malabsorption. It might not cause any problems at all. But it can cause symptoms like diarrhoea, bloating, wind, tummy pain and feeling sick. If it causes symptoms, it’s called lactose intolerance.
In the UK, around 8 in every 100 people are lactose intolerant. People with Colitis have a similar risk of being lactose intolerant as the general population. But people with Crohn’s may have a slightly higher risk. Some people with Crohn’s or Colitis only get symptoms of lactose intolerance during a flare-up.
Symptoms of lactose intolerance may be like flare-ups. So it’s important to talk to your IBD team before cutting out lactose.
Your IBD team can help you find out if you are lactose intolerant. If so, you can manage symptoms by following a low lactose or lactose-free diet. Some medicines also contain lactose. But do not stop taking any prescribed medicines without checking with your doctor or IBD team.
It is important not to cut foods out of your diet without talking to your dietitian or IBD team. It could mean you miss nutrients that your body needs.
For more information on healthy eating with Crohn’s or Colitis see our booklet on Food.
Drinking
If you have diarrhoea, you will lose more water than usual in your poo. So it is important to drink plenty of fluids. This could be drinks like water or diluted squash. Keep drinking small amounts of fluids often. You might need to increase the levels of salts and sugar in your body, as well as water. Oral rehydration solutions (ORS) are powders or tablets that are dissolved in water. They help the body replace water, salts, and sugar. You can buy oral rehydration solutions from most supermarkets and pharmacies. Your pharmacist can recommend a rehydration solution that is right for you.
If you have a high output stoma or short bowel syndrome, speak to your GP or IBD team to find out what type of rehydration would work best for you. You are more likely to need more salt than most store-bought rehydration solutions provide. Your GP or IBD team may recommend drinking an oral rehydration solution with a higher salt (sodium) level.
For more information on how to recognise and manage dehydration see our separate information resource: Dehydration.
If you have an ileostomy the contents of your bowel, called your stoma output, is usually quite liquid – like a paste or porridge. The output of a colostomy is usually semi-solid and can be like normal poo. But this varies depending on how much of your large bowel you have left. If you do not have much large bowel left, the output will be more liquid. The output of your stoma will vary and may increase or become more watery than usual if:
If this happens, keep drinking. You are likely to need rehydration therapy. Ask your pharmacist or IBD team. Eating foods that thicken your stoma output might help. Starchy foods like white rice, bread, pasta, noodles and peeled cooked potatoes are good. If your diarrhoea does not improve, your stoma nurse might suggest an anti-diarrhoeal medicine.
For more information see Living with a Stoma.
Frequent diarrhoea can cause sore skin around your bottom. Frequent washing and wiping of your bottom can also irritate the skin. The following tips may help prevent sore skin:
If your skin continues to feel sore or is broken, talk to your doctor or IBD team.
If you are worried about smells, you may wish to try odour neutralisers. These help to get rid of smells rather than just mask them. Products available include room sprays and toilet deodorisers.
We follow strict processes to make sure our information is based on up-to-date evidence and easy to understand.
Please email us at evidence@crohnsandcolitis.org.uk if:
You can also write to us at Crohn’s & Colitis UK, 1 Bishop Square, Hatfield, AL10 9NE, or contact us through our Helpline: 0300 222 5700
This page has been saved in your personal space. Go to “My Page” to view all saved pages.
We know it can be difficult to live with, or support someone living with these conditions. But you’re not alone. We provide up-to-date, evidence-based information and can support you to live well with Crohn’s or Colitis.
Our helpline team can help by:
Providing information about Crohn’s and Colitis.
Listening and talking through your situation.
Helping you to find support from others in the Crohn’s and Colitis community.
Signposting you to specialist organisations.
Please be aware we’re not medically or legally trained. We cannot provide detailed financial or benefits advice or specialist emotional support.
Please contact us via telephone, email or LiveChat - 9am to 5pm, Monday to Friday (except English bank holidays).
If you need specific medical advice about your condition, your GP or IBD team will be best placed to help.
Would you like to save the changes made to this page?
Your details were successfully saved.